General SurgeryPlanning the incision is very important in cardiothoracic surgery because it affects the results after surgery, the flexibility during surgery, the exposure, and the access. The pathophysiology dictates the operation; nevertheless, the feasibility of executing it effectively and safely is contingent upon the incision employed.
This page talks about the most common cardiothoracic incisions, including their anatomical landmarks, the reasons for doing them, and the things that impact which incision to choose.
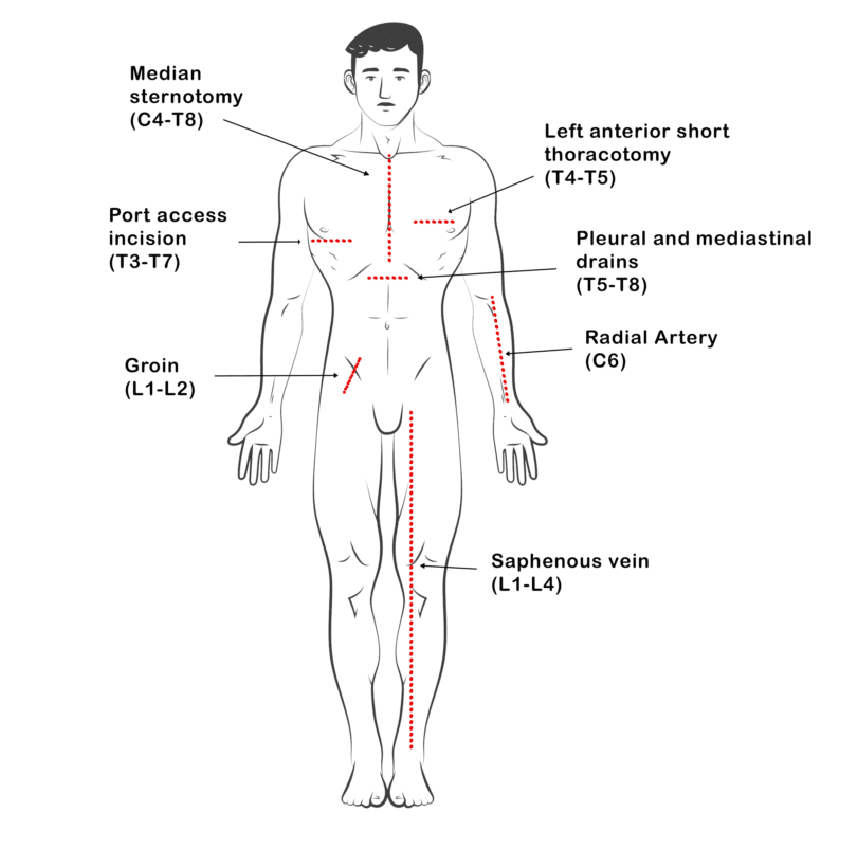
Multimodal Analgesia Strategies for Cardiac Surgery: A Literature Review – Scientific Figure on ResearchGate. Available from: https://www.researchgate.net/figure/Sites-of-incisions-in-cardiovascular-surgery-associated-with-postoperative-pain-C_fig1_383129778 [accessed 5 Sept 2025]
The Importance of Incision Technique in Cardiothoracic Surgery
The cardiothoracic incision is a deliberate selection rather than a mere incision. It is important to think about things like preserving muscle, recovering after surgery, exposure, organ accessibility, and the difficulty of the procedure. This article compares the most common incisions used in modern thoracic and heart operations.
1. Median Sternotomy: Frequent Clinical Applications for Mediastinal Access
The median sternotomy is still the most common way to get at:
- CABG stands for coronary artery bypass grafting.
- Fixing and replacing valves
- Surgery on the aorta’s root and arch
- Putting in a new heart
- Steps for congenital hearts
Anatomical Factors
Landmarks: xiphoid process to suprasternal notch
Method: Make a midline cut using an oscillating or sternal saw, and then do a vertical sternotomy.
The structures indicated are the sternum, the anterior mediastinum, the presternal fascia, and the tissue under the skin.
Advantages
- Extensive bilateral exposure of the heart and mediastinum
- allows access to the heart and main arteries at the same time.
- makes it easy to transfer between tasks, like going from fixing a valve to replacing it.
Limitations
- Risk of dehiscence, infection (mediastinitis), or ongoing sternal pain.
- Longer healing durations and cosmetic problems in people with a greater risk
2. Pacemaker Incision: Instructions for Putting Subcutaneous Devices in Place
utilized to replace generators, move subcutaneous leads, and put in pacemakers or ICDs.
Ways
Location of incision: left infraclavicular region
Length: 4–5 cm
Ways:
- In line with the clavicle, horizontal
- Oblique: follows Langer’s lines for a better look
- Deltopectoral: In difficult situations, follow the deltopectoral groove to get to the deeper parts.
Things to know about surgery
- A pocket is formed under the skin or muscle to put the gadget in.
- Venous access by an incision in the cephalic vein or a subclavian puncture
- Make sure the lead is securely attached and that the thoracoacromial vessels don’t get hurt.
3. Thoracotomy: Flexible Access to the Thoracic Cavity
Thoracotomy is necessary in both planned and emergency scenarios because it gives direct access to the pleural space, lungs, esophagus, pericardium, and main veins.
A. Posterolateral Thoracotomy
Reasons to do a Posterolateral Thoracotomy
- Lobectomy or Pneumonectomy
- Removal of malignancies from the chest wall
- Resection of the esophagus
- Draining or cutting off the edema
Ways to Study Anatomy
Position: Lying on one’s side
The incision should go from the mid-scapular line to the anterior axillary line, which is usually the fifth or seventh ICS.
Cutting through muscles:
- Dorsi Latissimus
- The anterior serratus (optional sparing)
- Trapezius and rhomboids (more visible)
Advantages
- The most exposure to the thorax’s structures
- Excellent access to the lower and back parts of the lungs
Limitations
- Pain after surgery, especially if the ribs are spreading a lot
- Longer recuperation time since the muscles are more disturbed
B. Anterolateral Thoracotomy
Signs that you need an anterolateral thoracotomy
- Thoracotomy in an emergency, such trauma
- Putting the left ventricular assist device (LVAD) in place
- Coronary or valve surgeries that are minimally invasive
Surgical Landmarks
Cutting at the fourth or fifth intercostal gap from the side of the sternum to the middle of the axilla
divides the pectoralis major from the serratus anterior.
Pros
- Fast access in emergencies
- helpful for redo thoracotomies and structures on the front
Trade-offs
- limited access to the back
- Comparing mild exposure to posterolateral
C. Axillary Thoracotomy
Reasons for Axillary Thoracotomy
- Pneumothorax, either primary or recurrent
- A lung biopsy or a wedge resection
- Chosen sympathectomy cases
Tech highlights
technique for keeping muscles
Cut between the front edge of the latissimus dorsi and the back edge of the pectoralis major
done through the fourth or fifth intercostal space
Pros
- prevents harm to muscles and keeps the shoulder working.
- Better results for the look
Cons
- minimal touch with the posterior thoracic or mediastinal tissues
- Not good for complicated resections
Summary Table: Comparative Summary
| Type of incision | access provided | muscle involvement | Common Uses | Comments |
|---|---|---|---|---|
| Median sternotomy | mediastinum and heart | Minimal (sternum midline) | CABG, valve, and transplant | The best way to do heart surgery |
| Pacemaker Cutting | region under the skin for inserting | an ICD without a pacemaker | Is it possible to use local anesthesia? | |
| Side Thoracotomy | The whole thoracic cavity | Extensive | Pneumonectomy, esophagectomy, and extensive lobectomy | maximal exposure, maximal illness |
| Anterolateral Thoracotomy | lung apex and front of the chest wall | Moderate | trauma thoracotomy and LVAD | Quick entrance, limited field |
| Axillary Thoracotomy | Upper thoracic cavity | Muscles that don’t hurt | pneumothorax and wedge biopsy | Great for looks 🧠 |
In conclusion: Choosing an Cardiothoracic surgery incision is not automatic; it is strategic.
The cardiothoracic incision is an important part of the process that influences every stage, from exposure and visualization to closure and healing. Even while procedures are moving toward robotic and minimally invasive approaches, it’s still important to know how to do things the old-fashioned way.
Surgeons always have to find a balance:
- Surgery exposure vs. invasiveness
- Keeping muscles vs being able to see them
- Cosmetic outcome versus complexity of operation
Each incision is depending on the patient’s anatomy, pathology, and how things are going throughout the surgery.
Important Lessons (Cardiothoracic Surgery INCISIONS)
- The cardiothoracic incision is necessary for both thoracic and cardiac operations to work.
- There is a unique clinical purpose for each procedure, from axillary thoracotomy to median sternotomy.
- Planning beforehand and knowing the anatomy well help get the best results and avoid difficulties.
Are you ready to get better at surgery? Leave a comment with your chosen incisions and recommendations for during surgery, or contact us for more evidence-based surgical information.